
What is Functional Neurological Disorder?

You may have never even heard of Functional Neurological Disorder (hereafter FND), but it’s one of the most common outpatient neurological diagnoses [1]!
As we learn more and more about how the brain adapts itself to our actions and our environment, we are also learning about maladaptive behaviors of the brain: when the brain changes ways in which we don’t want. Symptoms can include weakness, tremor, pain, dystonia, and many more. Read more below to learn about FND.
Laying the foundation: what is neuroplasticity?
To understand FND, it’s important to understand neuroplasticity. Neuroplasticity are physical changes to the brain. When we learn something new, be it a new dance move, how to knit, or multiplication tables, our brain makes the motor pathways between our muscles and different brain areas much more efficient; maybe what was once a single lane road becomes a super highway.
Further, the brain develops its own motor recipes to quickly recruit and coordinate all of the relevant parts of our body at once. Motor patterns are a lot like cooking recipes. To make or bake delicious food, you need both ingredients and the sequence of combining them into something delicious. A recipe for bread may include a handful of simple ingredients such as flour, yeast, salt, and water, but the sequence of arranging them into bread can be very complicated (how to tell when you’re done kneading the bread, how long to let the bread rise, baking temperature, and the agonizing wait for it to cool before slicing).
FND: undesireable neuroplasticity
With FND, the brain recruits movements, sensory systems, and more that are not necessary, or even detrimental, to the task at hand. For example, FND may increase activation of incorrect muscles, or reduce activation of correct muscles, prohibiting fluid walking. Sometimes, FND prohibits coordination of opposing muscle groups which may lead to tremor or dystonia. For some reason, the brain has learned to perform these tasks with unwanted ingredients in the brain’s recipe for the task.
Diagnosing FND: Can we “see” FND?
More and more, we are learning that image testing can be done to further confirm a diagnosis.
When an individual goes to a hospital suspecting they’ve had a stroke, doctors will often request CT and MRI imaging to see the stroke. In the case of a brain bleed, the CT will reveal the blood in the brain where it shouldn’t be. In an MRI and/or angiogram, we can visualize blockages in arteries. A common analogy used to distinguish FND from other conditions is that many neurological conditions can be seen on an image—called “hardware” injuries, whereas FND has been considered a “software” injury. While not as well studied as other conditions like stroke or spinal cord injury, there are emerging diagnostic studies that can be performed if FND is suspected; FND may not just be a so-called “software” concern.
In recent reviews of imaging research used to identify and study FND, these studies have found changes in the brain for individuals with FND via functional MRI [2,3]. In comparison to a traditional MRI, functional MRIs are taken while the individual performs tasks, measuring which parts of the brain “light up” during these tasks by monitoring blood flow changes in the brain. For individuals with FND, functional MRI studies have revealed altered activation of certain brain areas including the amygdala, and even heightened response in cortical areas to unpleasant stimuli. In addition to these possible blood flow changes to the amygdala, studies have shown that individuals with FND may also have increased activation at receptors associated with the amygdala [3].
In the image of brain areas below, the authors identify brain areas that demonstrate changes for individuals with FND as well as somatic conditions (SSD) [3]. Additionally, studies have also investigated brain volume of different brain areas, finding that a deep brain area called the insula may be negatively impacted by FND for those who have severe symptoms [4], similar to brain changes seen in other brain areas for individuals with PTSD.
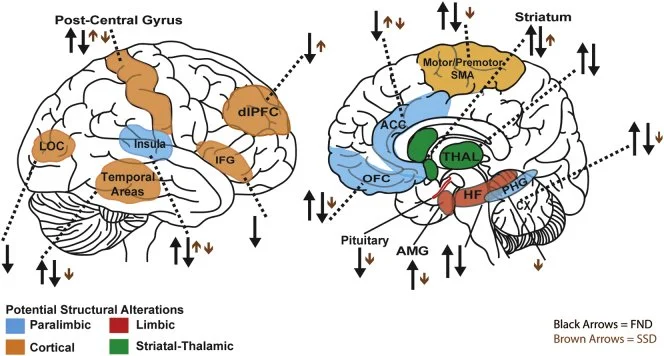
Interestingly, via these studies, researchers are learning more about both FND, as well as the functions of the brain. Some of these studies may reveal certain brain areas, including the thalamus, may play a larger role in the body than previously realized [3]. Additionally, other chronic conditions such as fibromyalgia and chronic pain disorders demonstrate similar brain changes to those seen in FND [3]; however, the question remains: are these brain changes a consequence of FND, or do these brain changes cause FND?
Unfortunately, many of these studies use smaller sample sizes, reducing applicability to a broader population, and at times have conflicting results. Many of these studies do not consider other co-existing conditions such as anxiety and depression. As more of these studies coalesce, with improved stratification between patient groups based on factors like age, symptomology, and severity of FND, we may come closer to definitive imaging techniques to diagnose FND, similar to how we diagnose someone with a stroke. As research continues onward, so too will diagnostics and treatment!
FND physical exam: clinical tests & measures
FND used to be considered a diagnosis of exclusion; we know now that FND has effective tests and measures (aside from imaging) that can further confirm a diagnosis, and are tests we often perform here at Headstrong. Symptoms of FND have a few things in common: they are entrainable, distractible, and variable.
The variability of symptoms can be surmised largely though the patient’s own observations. Is the FND “on” all the time? Do symptoms wax and wane? Are there triggers the individual has already identified?
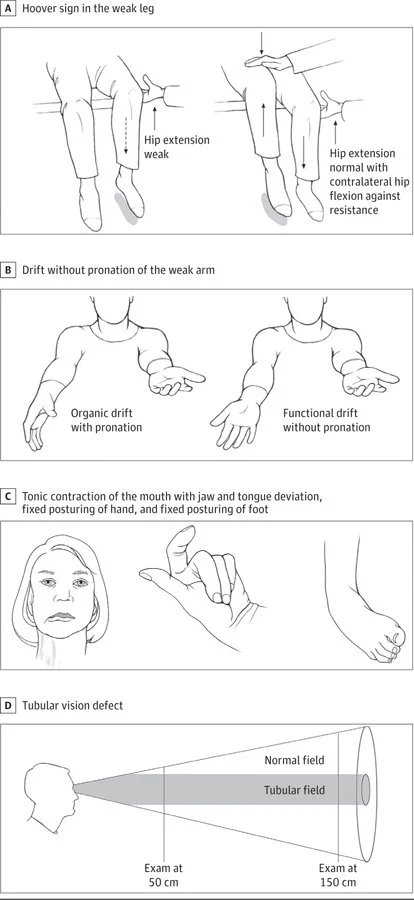
Distractability refers to alteration of the symptom with distraction. For example, a positive Hoover’s sign reveals that measured strength of one muscle changes if contracting the opposing muscle groups on the opposite side at the same time, such as left hip flexion weakness that improves with simultaneous right hip extension. See corresponding image from Espay et al. (2018) for visualization of the Hoover’s sign [5].
Tests that assess for entrainability of symptoms include the response of tremor speed when watching or performing a task at a different speed, meaning that the tremor can be “trained” to operate at a different frequency.
Clinicians identified the whack-a-mole sign [6], where suppression of unwanted movements such as tremor creates movements elsewhere, e.g suppressing tremor in one limb creates movement in trunk instead.
There are a variety of other “clinical pearls” that can lead to a diagnosis of FND including differentiation between FND and other motor symptoms such as dystonia. For example, dystonia that does not respond to a sensory trick is more likely to be caused by FND.
Treatment for FND
Even after a diagnosis is made, true for most conditions, part of pursuing treatment includes elucidating the cause of the diagnosis—for example, if someone experienced a head injury due to a fall, physical therapy may both the injury as well as the patient’s increased fall risk. Causes of FND are harder to pin down; in almost half of all cases of FND, the cause is idiopathic—we just don’t know! Some risk factors may include prior physical or emotional trauma, a preceding injury, or even recent illness with a virus like the common cold or COVID-19. What do we know is that external factors like environment, stress, diet, sleep regulation, and more can impact symptoms, regardless of cause.
If the brain has learned to do something incorrectly, we can use principles of motor learning and neuroplasticity to help teach the brain the correct way to perform the affected tasks. Current best practices use the OPTIMAL (Optimizing Performance through Intrinsic Motivation and Attention for Learning) theory of motor learning developed by Wulf & Lewthwaite [7]. In the OPTIMAL theory, the authors suggest that an individual’s attention may influence performance. When treating FND at Headstrong, we use this theory of motor learning to influence performance by redirecting attention away from the self (“interoception”), and towards an external focus. A good example would be focusing on kicking a ball to a particular target, rather than focusing on how the leg itself is or isn’t moving under our conscious control.
Step 1: Learn about the individual’s FND
The first step in treatment of functional neurological disorders is to learn what relieves, and aggravates, symptoms for the individual—what makes their FND “tick"—as FND affects each person differently! Therapists explore many factors that contribute to symptoms, which may involve a deep-dive into the day-to-day life of the patient, assessment of the scope of symptoms the patient experiences, as well as trial and error, exploring various modalities in clinic and at home to determine any impact on symptoms. A couple of examples include:
Symptoms can be triggered by autonomic causes, and for some, a co-diagnosis of postural orthostatic tachycardic syndrome (POTS). Managing heart rate and breathing changes, such as timed breathing and meditation, can be helpful in these cases. Good examples of activities to perform during flare ups make use of breathing strategies such as blowing bubbles or “box” breathing. Controlled breathing can directly affect the heart rate, blood chemistry, and nervous system activity.
For others, the sensory system plays a strong role in symptoms. In fact, many people with FND also have somatic disorders, altering reception of sensory information [3]. Someone with an overburdened sensory system may report light sensitivity, might comment that certain clothes trigger symptoms more, or that strong tastes or smells are unfavorable. Use of cold, heat, changing room lighting, even changing footwear can impact how an individual’s sensory system engages with their environment.

Step 2: Practice during conditions where symptoms are lessened
We take advantage of the fact that FND symptoms are distractible during treatment. People living with FND often endorse that hyperfocus on their symptoms can often make their symptoms worse. Can we redirect the brain’s energy away from how the body is performing—this so-called interoception—and instead make it focus on something else, reducing symptoms? As part of the OPTIMAL theory of motor learning, many rehabilitation protocols call for activities with a high degree of external focus—drawing attention away from the body, and placing that attention on the task performance itself. Some more examples include:
When walking, focus on kicking a ball instead of swinging the leg.
To restore altered balance, keep a pen laser focused on a target while performing a balance challenge.
When picking up an object, focus on timing the movement with breathing, to the beat of a song.
FND is not exclusive in its response to external focus! People with Parkinson’s often benefit from sound cueing when taking steps, walking to the beat of a metronome, or a visual cue e.g as is provided by a U-Step walker laser, to reduce the impact of bradykinesia on their walking ability.
One of the tenets of neuroplasticity includes repetition of practice: if you use it, you improve it [8]. When symptoms are lessened, it’s all about repetition, repetition, repetition! Here at Headstrong we emphasize repeated performance of the modified activity to help re-train the brain, encouraging the original, tried-and-true, recipe for movement before FND changed the recipe. Eventually, these aids are no longer needed as the brain learns more and more through repeated practice the favored way of performing a task.
References
Functional (psychogenic) movement disorders: merging mind and brain. Edwards, Mark J et al. The Lancet Neurology, Volume 11, Issue 3, 250 - 260
Perez DL, Nicholson TR, Asadi-Pooya AA, et al. Neuroimaging in Functional Neurological Disorder: State of the Field and Research Agenda. Neuroimage Clin. 2021;30:102623. doi:10.1016/j.nicl.2021.102623
Bègue I, Adams C, Stone J, Perez DL. Structural alterations in functional neurological disorder and related conditions: a software and hardware problem?. Neuroimage Clin. 2019;22:101798. doi:10.1016/j.nicl.2019.101798
Perez DL, Williams B, Matin N, et al. Corticolimbic structural alterations linked to health status and trait anxiety in functional neurological disorder. J Neurol Neurosurg Psychiatry. 2017;88(12):1052-1059. doi:10.1136/jnnp-2017-316359
Espay AJ, Aybek S, Carson A, et al. Current Concepts in Diagnosis and Treatment of Functional Neurological Disorders. JAMA Neurol. 2018;75(9):1132-1141. doi:10.1001/jamaneurol.2018.1264
Park JE, Maurer CW, Hallett M. The "Whack-a-Mole" Sign in Functional Movement Disorders. Mov Disord Clin Pract. 2015;2(3):286-288. Published 2015 May 25. doi:10.1002/mdc3.12177
Wulf G, Lewthwaite R. Optimizing performance through intrinsic motivation and attention for learning: The OPTIMAL theory of motor learning. Psychon Bull Rev. 2016;23(5):1382-1414. doi:10.3758/s13423-015-0999-9
Kleim JA, Jones TA. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. J Speech Lang Hear Res. 2008;51(1):S225-S239. doi:10.1044/1092-4388(2008/018)